Revista Peruana de Investigación en Salud, ISSN: 2616 - 6097 https://doi.org/10.35839/repis.5.2.930
Invasive Mechanical Ventilation of COVID-19 ARDS Patients
Ventilación mecánica invasiva de pacientes con SDRA por COVID-19
Vijay Singh1, Shibu Sasidharan1,a, Abdul Naseer2, Harpreet Singh-Dhillon1, Babitha Manalikuzhiyil3, Suneeta Singh1, Divya Sinha4, Gurpreet Kaur-Dhillon5, Shalendra Singh6
1Level III UN Hospital, Goma, DR Congo
2Naval Hospital, Goa, India
3Ojas Hospital, Panchkula, India
4Sai Sukhda Hospital, Bareilly, India
5166 Military Hospital, Jammu, India
6AFMC, Pune, India
Corresponding author E-mail:shibusasi@gmail.com
Orcid ID: ahttps://orcid.org/0000-0003-2991-7595
Reception date: january 27, 2021
Approval date: april 07, 2021
Abstract
The purpose of this review article is to analyse evidence on the use of ventilatory strategies and associated cointerventions in adult patients with COVID-19 induced acute respiratory distress syndrome (ARDS) and to provide treatment recommendations based on these interventions. For each recommendation mentioned, it is important to consider the quality of the evidence reviews thoroughly before applying these recommendations to specific clinical situations or policy decisions. No guideline or recommendations can consider all the compelling clinical features of individual patients, as they are unique. Thus, it is imperative that clinicians, patients, policy makers, and other stakeholders should not regard these recommendations as mandatory. However, this review article, impartially discusses the nuances of treatment available and management protocols followed in many centres around the world for the consumption of all treating physicians.
Keyword: Covid-19, mechanical ventilation, ICU.
Resumen
El propósito de este artículo de revisión es analizar la evidencia sobre el uso de estrategias ventilatorias y cointervenciones asociadas en pacientes adultos con síndrome de dificultad respiratoria aguda (SDRA) inducido por COVID-19 y brindar recomendaciones de tratamiento basadas en estas intervenciones. Para cada recomendación mencionada, es importante considerar la calidad de las revisiones de la evidencia a fondo antes de aplicar estas recomendaciones a situaciones clínicas específicas o decisiones políticas. Ninguna guía o recomendación puede considerar todas las características clínicas convincentes de los pacientes individuales, ya que son únicas. Por lo tanto, es imperativo que los médicos, los pacientes, los responsables políticos y otras partes interesadas no consideren estas recomendaciones como obligatorias. Sin embargo, este artículo de revisión analiza de manera imparcial los matices del tratamiento disponible y los protocolos de manejo seguidos en muchos centros alrededor del mundo para el consumo de todos los médicos tratantes.
Palabras clave: Covid-19, ventilación mecánica, UCI.
Introduction
A novel coronavirus was identified in Wuhan, China in December 2019, causing atypical pneumonia and rapidly spreading resulting in a pandemic. The World Health Organization designated the term COVID-19 (Coronavirus Disease 2019) for this pandemic. COVID-19 is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The major morbidity and mortality from COVID-19 is attributed to the acute viral pneumonitis that progresses to acute respiratory distress syndrome (ARDS).
Definition of ARDS: COVID-19 ARDS (CARDS) is diagnosed when someone with a confirmed COVID-19 infection meets the Berlin 2012 ARDS diagnostic criteria(1), which include:
(i) Acute hypoxemic respiratory failure; (ii) Presentation within 1 week of worsening respiratory symptoms; (iii) Bilateral airspace disease on chest x-ray, computed tomography (CT) or ultrasound that is not fully explained by effusions, lobar or lung collapse, or nodules; and (iv) Cardiac failure is not the primary cause of acute hypoxemic respiratory failure This article will attempt to discuss the management of patients who develop ARDS due to COVID-19.
Methods We convened an interprofessional panel with a broad sample of anaesthesiologists, clinical epidemiologists, paediatricians, internal medicine specialists, psychiatrist, radiologist and methodo-logists to evaluate various studies with respect to COVID-19. We then had a face-to-face discussion on the same in our hospital before summarising our understanding. We evaluated existing systematic reviews from our search in MEDLINE, EMBASE, Cochrane Registry of Controlled Trials, Database of Abstracts of Reviews of Effects (OvidSP), CINAHL (EBSCOHost), and Web of Science (Thomson Reuters) from the date of the last systematic review to December 2020, without language restrictions. Panel members were also asked to highlight any additional studies not identified by the search. Recommendations are either “strong” or “conditio-nal” according to the GRADE approach(2). We used the GRADE phrases “we recommend” for strong recommendations and “we suggest” for conditional recommendations.
Manuscript was prepared by the writing committee (S.S, V.S) drafted the guideline document for subsequent electronic review by the entire panel. The entire panel had the opportunity to correct factual or interpretative errors. The final approved version was then submitted.
Oxygenation & ventilation for CARDS (CARDS) patients CARDS follows an anticipated time course, with a median time to intubation of 8 - 10 days after symptom onset (3). It is therefore imperative to constantly monitor patients for the development of ARDS as the day of infection progresses. The primary strategy for COVID-19 patients is supportive care, which includes oxygen therapy for hypoxemic patients. Oxygen therapy is instituted if respiratory rate is of 30 breaths/min or above and/or SpO2 of ≤93% on breathing air(4).
COVID-19 patients sometimes present with “silent or happy hypoxia” (atypical clinical features like feeling of calm and sense of wellbeing even in presence of significant level of hypoxia). The reason for this is the presence of low carbon dioxide levels (severe hypocapnic hypoxia) in blood, typically found in high altitude sickness(5). Atypical findings like these confuse treating physicians to intubate or not to intubate. Mechanical ventilation of COVID-19 patients with ARDS (CARDS) is an unprecedented and challenging task as these patients usually have non homogenous lung pathology that requires a targeted lung-protective ventilation strategy to improve outcome. Most patients of CARDS require timely institution of mechanical ventilation. Undue delay in intubation and invasive mechanical ventilation will be detrimental to the patient and the risk of contagion spread to healthcare workers is high(6). A low threshold for intubation should be considered if the clinical condition of the patient deteriorates even with increase oxygen supplemen-tation at high flow and at high FiO2.
Non invasive modes High-flow nasal oxygen therapy (HFNO) is used as first-line treatment(3) for respiratory failure and mild-moderate ARDS. Non-Invasive Ventilation (NIV) is only recommended for patients with failed HFNO. NIV provides benefit via PEEP, to patients with mild-moderate ARDS by reducing the respiratory load and intubation rate, but it can cause significant aerosol generation.
High-flow nasal cannula (HFNC) for HFNO is effective in improving oxygenation, but due to reports of high amount of aerosol dispersion it was not recommended initially. However further studies in patients with acute hypoxemic respiratory failure, HFNC was proven to avoid intubation compared to conventional oxygen devices, and the scientific evidence of generation and dispersion of bioaerosols via HFNC showed a similar risk to standard oxygen masks. HFNC prong with a surgical mask on the patient's face is thus a reasonable modality to benefit hypoxemic COVID-19 patients and avoid intubation(7). HFNC therapy essentially is an oxygen supply system capable of delivering up to 100% humidified and heated oxygen at a flow rate of up to 60 litres per minute. All settings are controlled independently allowing for greater confidence in the delivery of supplemental oxygen as well as better outcomes when used(8).
Prone Positioning for Non-intubated Patients : Although prone positioning has been shown to improve oxygenation and outcomes in patients with moderate-to-severe ARDS who are receiving mechanical ventilation, there is less evidence regarding the benefit of prone positioning in awake patients who require supplemental oxygen without mechanical ventilation(9).
Precautions and procedures followed while intubation of COVID-19 patients Airway management and intubation in COVID-19 patients is an aerosol generating procedure and is associated with increased risk of viral transmission to the health care providers. Hence, a high level of attentiveness is necessary to prevent infection when intubation is performed. Safety of patients and health care workers can be ensured by the following precautionary measures(10).
1. Health care professional should take airborne precautions with a standard level 3 protection to be donned while performing intubation. The recom-mended sequence for donning of personal protective equipment (PPE) is as follows: hand sanitisation/washing → head cap → protective N95 mask → surgical masks → full body isolation gown → disposable inner gloves → goggles → protective clothing → disposable outer gloves → shoe covers → disposable gown → disposable outermost gloves → full head hood or face shield(11). 2. For intubation, the acronym OH–MSMAID (Oxygen, Helper, Monitor, Suction, Machine, Airway devices, Intravenous access, and Drugs) can be used to ease of remembrance(12). 3. Tracheal intubation should be performed by the most experienced anaesthesiologist, in an airborne infection isolation room, preferably in a negative pressure room to ensure patient safety and HCW (Health care worker). 4. The number of health care provider in the room prior to intubation should be limited. 5. Use 3-5 minutes of pre-oxygenation with 100% oxygen is mandatory as these critical patients have poor oxygen reserve(13). 6. Spontaneous ventilation should be preserved and as much as possible, assisted bag mask ventilation during preoxygenation should be avoided. 7. RSI (rapid sequence intubation) technique is to be recommended to avoid manual ventilation of the patient's lungs and prevent potential aerosolization of the virus from the airways. A COVID aerosol barrier intubation box can be used to shield aerosols(14). 8. Use both hands to hold the mask to ensure a tight seal using the V-E technique rather than the C-E technique with one hand. 9. Video laryngoscope should be preferred for intubation as it increases the distance between the patient and anaesthesiologist. 10. Airway management should be safe, accurate and should be done within 15-20 seconds. 11. After tracheal intubation, clamp the ETT (endotracheal tube) and inflate the cuff before instituting mechanical ventilation. 12. Viral and HME filter must be connected between endotracheal tube and circuit. 12. Proper tube placement can be confirmed by EtCO2 monitoring, visible bilateral chest rise and routine 5 point auscultation is preferably avoided to confirm tube placement. 13. Supraglottic airway devices (SGAD) should be used in CICO (Can`t intubate and can`t oxygenate) situations only and bedside tracheostomy should be considered as early as possible. 14. If intubation is required while transporting patients with CARDS, it must be ensured that all protocols mentioned above should be adhered to(15).
Mechanical ventilation Mechanical ventilation of COVID-19 patients with ARDS is challenging as these patients usually have a non-homogenous lung pathology. This requires a targeted lung-protective ventilation strategy to improve the outcome.
Indications for Mechanical Ventilation The indications for mechanical ventilation in COVID-19 are as follows(7):
1. Acute hypoxic respiratory failure with severe respiratory distress. 2. Worsening hypoxia associated with increased laboured breathing. 3. Increase work of breathing associated with use of accessory muscles of respiration. 4. Failure to maintain Spo2 >90% with >50 L/minute of high flow oxygen with HFNO or with maximal supplemental oxygen(16). 5. Hypoxia with altered mental status and failure to maintain airway patency. 6. Patient with multiorgan failure, persistent hemodynamic instability requires vasopressor support, or those with multiple comorbidities like (DM, Cardiovascular disease, hypertension, advanced age, frailty, cancer or chronic respiratory disease). 7. Arterial PH <7.3 with PaCO2 > 50mm Hg. 8. PaO2/FiO2 < 200 (17). 9. High respiratory rate with persistent thoracoab-dominal asynchrony or paradoxical respiration. 10. Low ROX index (< 4.88) with patient on HFNC. (The ROX index(18) defined as the ratio of Spo2/FiO2 to respiratory rate and it has been used as a predictor of the intubation need in patients received HFNC oxygen therapy. A ROX index ≥ 4.88 after HFNC initiation is associated with a lower risk for intubation.)
Indications for intubation and mechanical ventilation in COVID-19 patients are not limited to the above mentioned conditions and should be case-specific, and at the discretion of the treating physician(19).
Ventilatory strategy for CARDS The optimal time to intubate COVID-19 patients is still not clear. Mechanical ventilation should be considered if a COVID-19 patient develops moderate to severe ARDS (PaO2/FiO2 < 200) to prevent P- SILI (Patient self-induced lung injury) and viral transmission to health care provider [6]. Endotracheal intubation and invasive mechanical ventilation are to be considered on priority in ARDS patients who are acutely deteriorating in spite of supplemental oxygen therapy with HFNC. Non-intubated spontaneously breathing ARDS patients are at increased risk of P-SILI due to high intake of inhaled tidal volume. Therefore, oesophageal pressure measurement by manometer can be used in spontaneously breathing, non-intubated patients to estimate the time for intubation(20). The risk of infection to the HCW remains a concern. The oesophageal pressure between 5 to 10 cmH2o is generally well tolerated. However, if pressure goes more than 15 cmH2O, then risk of P-SILI increases and therefore intubation should be carried out as soon as possible. If oesophageal manometry is not available, then change in CVP (centre venous pressure) with respiration or clinical assessment of excessive inspiratory effort for increased work of breathing to be considered(21).
Mortality is very high (67%) for CARDS patients on mechanical ventilation (22). An inappropriate ventilatory strategy in ARDS patients can lead to VILI (Ventilator induced lung injury) which includes barotrauma (high airway pressure), volutrauma, atelectrauma, biotrauma, myotrauma (diaphragmatic injury) and oxytrauma (oxygen free radicles).
Non COVID -19 ARDS has two sub phenotypes identified based on the ARMA and ALVEOLI trial. They respond differently to PEEP, liberal fluid therapy and can be identified with notable precision using four biomarkers: interleukin-6, interferon gamma, angiopoietin 1/2, and plasminogen activator inhibitor-1 (23)(24)-
(a) Hyperinflammatory type- This type is associated with higher levels of inflammatory biomarkers, high vasopressor use, high sepsis, lower serum bicarbonate and have worst outcome in terms of mortality, ventilator free days and organ-free days. It responds to high PEEP and conservative fluid therapy. (b) Hypo inflammatory type- It responds to low PEEP and liberal fluid therapy(25) .
Preliminary anecdotal reports on CARDS mentioned(26)(27) that in the early phase of COVID-19, atypical ARDS features are more common (severe hypoxemia with high compliance and low lung recruitability) while in the later phase of disease, classic ARDS features are more common (low lung compliance and high alveolar recruitability). Gattinoni et al.(26)(28) also reported that COVID-19 pneumonia is of two types and their management varies in terms of ventilatory management –
a. Type L – characterised by low elastance, high compliance, low lung weight, low lung recruitability, and low ventilation-to perfusion (V/Q) ratio. b. Type H- characterised by high elastance, low compliance, high lung weight, high lung recruitability, and high right-to-left shunt. This type of pneumonia has features like typical ARDS.
Currently there is no consensus on ventilatory management of CARDS patients. Hence, the ventilatory strategy for ARDS patients i/e low tidal volume ventilation, best suits for managing CARDS also. Salient features of the same are enumerated below:
(1) Lung protective ventilation(29)- Several randomized control trials and meta-analyses have reported survival benefits from low tidal volume lung protective ventilation. After implementation of low tidal volume ventilation in ARDS patients monitor auto-PEEP & ventilator dyssynchrony has to be monitored (30). There is no single mode of ventilation which is markedly better than other modes in managing ARDS patients(31). However, most clinicians prefer to use volume-limited assist-control mode for ventilating ARDS patients(30). Modes of ventilation like Airway pressure release ventilation (APRV) may be also be used based on physician's expertise(32). High frequency oscillatory ventilation is best avoided due to risk of aerosol spread and has shown no mortality benefit in ARDS patients(12). Even, Pressure-regulated volume control is also not an accepted mode of ventilation in ARDS patients due to high tidal volume delivery surpassing the lung-protective ventilation target. The following initial ventilatory settings (Table 1) are recommended in COVID-19 patients:
Table 1 Ventilator settings for lung protective ventilation
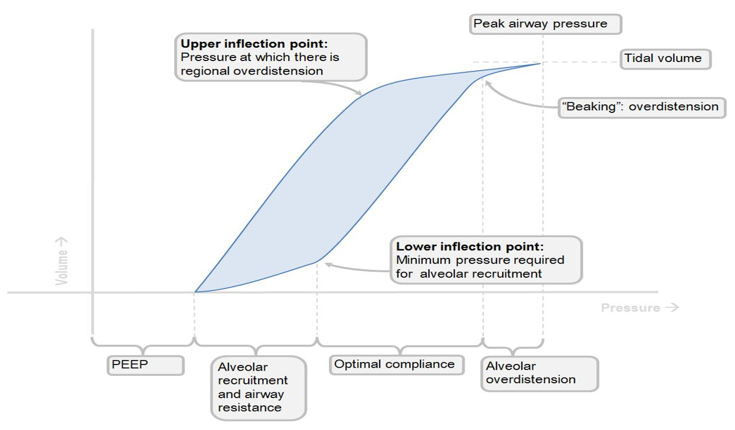
(2) Role of PEEP in CARDS- There is an ambiguity with optimal PEEP for CARDS patients. Using higher PEEP (any PEEP >10cm H2O) was not recommended based on the heterogenicity of lung involvement in COVID-19 patients (with simultaneous existence of severely affected areas with non-affected areas in the lung). However, surviving sepsis campaign guidelines on management of critically ill adults from COVID-19, European intensive and critical care guidelines, advise PEEP > 10cm H2O for management of ARDS due to SARS-CoV-2. Titrations need to done by checking for lung compliance of COVID-19 patients. If it is high or normal with presence of hypoxemia which is more common in L- Phenotype, then use of PEEP less than 10 cm H2O is recommended to avoid over-distention of normal healthy alveoli. However, if compliance is low, which is more common in H- Phenotype of COVID-19 pneumonia likely also seen in ARDS, then use PEEP just above the lower inflection point on pressure volume loop on the ventilator to recruit collapsed alveoli, and prevent atelectasis and thereby, improve oxygenation. Monitor for alveolar over-distension by observing 'Beaking' pattern on pressure- volume loop which can be corrected either by decreasing tidal volume or PEEP (Figure 1).
Figure 1 Pressure-Volume loop with lower inflection point
(3) FiO2/PEEP ladder for oxygenation - ARDSNet trial (33) recommends to consider two types of FiO2/PEEP ladder to achieve the goal of PaO2 > 55 mm Hg in ARDS patients and to avoid the side effects of hyperoxia. D Trasy et al's study(34) recommends use of FiO2/PEEP index ≤7 which is similar to the ARDSNet trials of minimum FiO2/PEEP settings (35%/5 cmH2O). The details of FiO2/PEEP ladder are tabulated below in Table 2,3 -
(a) Higher FiO2/Lower PEEP
Table 2 Higher FiO2/Lower PEEP
(b) Lower FiO2/higher PEEP
Table 3 Lower FiO2/Lower PEEP
Once the initial ventilator settings are entered, then the following parameters are monitored along with their target levels-
(a) Plateau pressure- Plateau pressure should be below 30 cm H2O. It is defined as the pressure that is maintained in the alveoli when there is no airflow. It is slightly lower than Ppeak pressure and is measured by adding an inspiratory pause of 0.5 to 1 second on volume control mode showing pressure time scalar. (b) Driving pressure- It is measured by formula : Driving pressure= (Pplat pressure – PEEP) This pressure should be below 15cm H2O and is achieved by either decreasing tidal volume (at the risk of development of hypercapnia) or by increasing PEEP (risk of overdistention of alveoli). Therefore, PEEP and tidal volume should be carefully titrated to keep driving pressure low. (c) Compliance– It is a measure of ease of distensibility of lung elastic tissue. The easier a lung able to expand or stretch, more will be its compliance. Normally, the total compliance of both lungs in an adult is about 200 ml/ cm H2O. Low compliance is usually found in ARDS patients with stiff lung. There are two types of lung compliance-
1.Static compliance =
2. Dynamic compliance =
It represents pulmonary compliance during active inspiration and depends upon peak inspiratory pressure (PIP). PIP depends on airway resistance. COVID -19 Pneumonia is a L phenotype(26)(28) usually with high compliance (> 40ml/cm H2O). So, a low PEEP and high tidal volume up to 8-9ml/kg (if hypercapnia present) is advised. H- phenotype pneumonia is managed like ARDS with lung protective ventilation (low tidal volume (4-6ml/kg) along with high PEEP). Therefore, it is essential to look for respiratory compliance of these patients prior to make any adjustment in ventilatory settings.
(d) P0.1 (Airway occlusion pressure)- It is defined as the pressure generated in the airways during the first 100 msec of an inspiratory effort against an occluded airway. This can be measured in most modern ventilators. The normal value of P0.1 (in spontaneously breathing patients) is about 1 cm H2O. However, in mechanically ventilated patients' values above 3.5 cm H2O are associated with increased effort. Therefore, airway occlusion pressure value in CARDS patients should be kept less than 3.5 cm H2O to obtain a ventilatory strategy protective for the lung (to prevent it from VILI and diaphragmatic injury (Myotrauma)).
(3) Target goals of mechanical ventilation(35)-
1. Target SPO2 = 90-94% 2. PaO2 > 55 mm Hg. 3. pH > 7.25 4. FiO2 < 0.4 5. PaO2/FiO2 > 300mm Hg.
(4) Subsequent ventilatory settings- Subsequent ventilatory settings is decided by dynamic assessment of Pplat pressure, driving pressure, compliance, and ABG (pH, oxygenation level) as done in non-CARDS(33). Some working guidelines are as under:
(a) If Pplat ≤30 cm H2O, tidal volume (6 mL/kg) and normal PH- No further adjustments. (b) If Pplat >30 cm H2O and tidal volume (6 mL/kg or higher) – Decrease tidal volume to 5ml/kg if required, further decrease it to 4ml/kg. Consider increase in respiratory rate till up to 35/min to maintain an acceptable minute ventilation. (c) If ventilator dyssynchrony present with Pplat <25 cm H2O and tidal volume (<6 mL/kg)- increase tidal volume to 1 mL/kg increments up to 8ml/kg to achieve Pplat >25 and ≤30 cm H2O. (d) If pH > 7.45 with respiratory alkalosis- decrease respiratory rate to target pH 7.25 -7.45. (e) If pH < 7.25 with respiratory acidosis- increase respiratory rate up to 35/min (concern auto-PEEP) to target pH 7.25 -7.45. (f) If pH < 7.15 with respiratory acidosis- after maximum respiratory rate (35/min), increase tidal volume in 1ml/kg increments (target Pplat < 30 cm H2O and PH 7.25 -7.45) or administer NaHCO3 if metabolic acidosis also present.
(5) Other adjuvant therapies:
(a) Sedation and analgesia Propofol and midazolam are two most commonly used drugs for ICU sedation of mechanically ventilated patients and may be useful for sedation of CARDS patients who are on mechanical ventilation. Melatonin has been considered as a supportive therapy to improve sleep in COVID-19 patients in ICU, although more studies are required to validate this recommendation(36). In an ongoing pandemic like COVID-19, there is an acute shortage of sedatives and analgesics. Thus, some physi-cians/intensivists have evaluated inhalational volatile anaesthestic agents as an alternative for sedation. Volatile anaesthetic agents like isoflurane & sevoflurane have advantages beyond sedation. This includes decreased airway resistance, bronchodilatation (in dose dependent manner), improved oxygenation, reduction of proinflam-matory markers and decreased lung epithelial injury(37). However, they have not shown improvement in length of ICU stay or mortality benefit. Thus, further clinical studies or RCTs are required to interpret favourable outcome(38). To administer inhaled anaesthetics in ICU trained staff and anaesthesia machine / ventilator with miniature vaporizer and scavenging systems should be available. The main purpose of using sedation in COVID-19 patients with ARDS is to ensure patient comfort, alleviate anxiety, and to avoid ventilator asynchrony.
Two tools used to assess level of sedation in ICU patients are:
1. Richmond Agitation Sedation Scale (RASS)- A target of -3 to -4 points is kept for deep sedation of mechanically ventilated ICU patients. A target of -5 is required when patients receive NMBA (to prevent patient- ventilator asynchrony) (39)(40). 2. Riker Sedation- Agitation Scale (SAS)- A target of 2 points is required to achieve deep sedation and SAS 1 is required for very deep sedation like patients on prone ventilation or ECMO. Light sedation by Dexmedetomidine with target value of SAS 3 - 4 may be suitable for COVID-19 patient on HFNC oxygen supplement therapy to control the physiological stress response(39).
In resource deficit conditions, processed EEG devices (Bispectral index (BIS), entropy and narcotrend-derived variables) can be utilized as a valuable monitoring device to reduce drug utilisation and to monitor need for sedatives (41)(42). Besides sedation, providing adequate analgesia is also equally important. A combination of agents (ketamine, fentanyl, morphine, hydromorphone, dexmedetomidine, remifentanil, sufentanil) may be considered as per requirement of the patient. According to PADIS guidelines(43), remifentanil and sufentanil are the analgesics of choice.
Three pain scoring scales are routinely used to assess the subjective nature of pain in ICU (39)-.
1. Numeric rating scale (NRS)- Target range < 4. This may be considered for non- ventilated spontaneously breathing COVID-19 patients who can express pain themselves. 2. Behavioral pain scale (BPS)- Target range < 5 and can be used for mechanically ventilated patients. 3. Critical care pain observation tool (CPOT)- Target range < 3 and can be used in critically ill patients on invasive ventilation.
(b) NMBA (neuromuscular blocker agents)- No clinical trials have been conducted on the use of NMBA in COVID-19 patients with ARDS. However, several intensive and critical care societies worldwide(44)(45) have made recommendations on the use of NMBA to improve oxygenation and to reduce ventilator dyssynchrony in ARDS patients. NMBA may be used in boluses (but not in continuous infusion) in moderate to severe ARDS patients with refractory hypoxemia (PaO2/ FIO2 < 120 mmHg) to facilitate oxygenation, improved lung ventilation(46) and to avoid critical illness neuropathy. Routine use of neuromuscular blocking agents is not advised as it doesn`t reduce duration of mechanical ventilation and there is no survival benefit in ARDS patients. For intubation of CARDS patients, rapid sequence induction technique practiced, and therefore, succinylcholine and rocuronium are the preferred choice of NMBA in COVID-19 patients(10)(47). However, for inter-mittent boluses, rocuronium, vecuronium, and atracurium are more preferred compared to succinylcholine. TOF monitoring in ICU can contribute to better utilisation of NMBA [31].
(c) Recruitment manoeuvres (Rms)- Recruitment manoeuvres with high PEEP are used to improve oxygenation in CARDS patients by increasing transpulmonary pressure to open atelectatic or collapsed alveoli. Until now, no studies have found out the exact role of recruitment mano-euvres (RMs) in patients with ARDS secondary to SARS-CoV-2. Surviving Sepsis Campaign guidelines(48)advise to use RMs with high PEEP to open collapsed alveoli and against the use of incremental PEEP titration RMs in COVID-19 patients. Use of incremental PEEP for recruitment manoeuvres is discouraged in favour of RMs with high PEEP in COVID-19 patients. WHO interim guidelines also advise use of intermittent recruitment manoeuvres with high PEEP to improve oxygenation in ARDS due to COVID-19. It is essential to watch for hypotension, desaturation, and lung barotrauma during RMs. The two types of RMs used in ARDS patients are as under (48)-
1. Traditional RMs – High level of CPAP (35-40 cm H2O) along with prolonged inspiratory pause (40sec) is preferred in COVID-19 patients. 2. Incremental PEEP titration RMs- In this RM, incremental PEEP is used from 25 to 35 to 45 cm H20 for 1–2 min each and not recommended for COVID-19.
(d) Administration of Steroids WHO recommends(29) administration of steroids in CARDS patients on mechanical ventilator who have developed septic shock and require increasing dose of vasopressors to maintain MAP > 65 mm Hg. Inj. Hydrocortisone 200mg/day or prednisolone 75mg/day is adviced. Surviving Sepsis Campaign guidelines(48) suggest use of systemic corticos-teroids in CARDS and advise to use corticosteroids in lower doses for shorter duration. However, routine use of corticosteroids for COVID-19 mechanically ventilated patients with respiratory insufficiency without ARDS is not recommended.
(e) Anti-Thrombotic therapy for CARDS Antiplatelet therapy is associated with reduced mortality and lower incidence of ARDS/ALI in critically ill patients, particularly those with predisposing conditions such as high-risk surgery, trauma, pneumonia, and sepsis(49). Accordingly, it may act as a prophylactic agent and/or as a treatment in critically ill patients with the above mentioned conditions. Importantly, with a large number of the critically ill population, even a low rate of avoidable harm will be associated with massive preventable deaths. Consequently, it is imperative to identify the role of antiplatelet treatment as an adjunctive therapy in critically ill patients.
(f) Fluid therapy WHO [19] and Surviving Sepsis Campaign guidelines(48) recommends use of conservative or restricted fluid therapy, over liberal fluid. It has shown to decrease the number of days on ventilator and shortens ICU stay. Surviving Sepsis Campaign guidelines used indirect evidence and recommends use of dynamic parameters (Skin temperature, capillary refill time, serum lactate, stroke volume variation (SVV), pulse pressure variation (PPV) and stroke volume change with passive leg raising) over static parameters (CVP) to assess fluid respon-siveness in COVID-19 patients with septic shock.
(g) Nutritional support According to ESPEN expert statements(50) and ESPEN guidelines(51), the nutritional support for SARS CoV-2 infected patients in ICU are as under-
1. Malnutrition assessment in polymorbid patients- MUST criteria & NRS criteria must be used to check/screen individuals with COVID-19 for malnutrition . 2. Patients on NIV- Peripheral parenteral nutrition is preferred as NIV along with enteral feed is associated with complications like stomach dilatation (prone for aspiration) and ineffective ventilation though due to air leak from the side of the facemask. 3. For patients on HFNC - Oral nutritional supplements can be after assessing the nutritional status of COVID-19 patient or start enteral feed if oral feed is not possible. 4. Patients on ventilator –
a) Early enteral feed (within 48hrs of ICU admission) through nasogastric tube is favoured over late enteral and early parenteral feed. b) Post pyloric feed to be started in patients prone for gastric aspiration or in cases of gastric intolerance after prokinetic drugs. c) Parenteral nutrition can be administered within 3-7 days if contraindications to enteral nutrition are present. d) Indirect calorimetry, VO2 or VCO2 estimation is recommended to guide daily energy expenditure (EE). If not available, weight-based equations to be used to estimate daily calorie expenditure (20–25 kcal/kg/day) e) Enteral nutrition can be given to prone ventilated patients and is verified to be safe in CARDS. f) In the early phase of illness (first week), hypocaloric nutrition (not exceeding 70% of EE) should be administered. g) After the early phase of acute illness, isocaloric nutrition is recommended over hypocaloric nutrition. h) In frail patients, protein administration (1.3 g/kg /day) can be considered progressively during critical illness. i) For obese patients, requirement of protein is 1.3g/kg (adjusted body weight)/day. Adjusted body weight = Ideal body weight + 0.33 X (actual body weight - ideal body weight) j) EN can be delayed in haemodynamic unstable patients with shock on vasopressors, severe hypoxemia, and severe acidosis.
5. Post-extubation patients- Texture adapted food to be considered orally and if dysphagia is present (which is most common in post-extubation), administer enteral nutrition.
(h) Management of septic shock In the absence of direct evidence on COVID-19 patients and septic shock, WHO interim guide-lines(29) and Surviving Sepsis Campaign guidelines (48) recommends use of crystalloid intravenous balanced fluids like Normal Saline, Ringer`s Lactate as fluid bolus (1liter over 30min or faster) for septic shock to check for fluid respon-siveness. Hypotonic fluids, colloids, hydroxyethyl starches, gelatin, dextrans and albumin should be avoided for resuscitation. If there is no fluid response and signs of fluid overload appear like crackles on auscultation, then discontinue the fluid and consider using vasopressors. In vasopressors, Norepinephrine is the drug of choice followed by vasopressin & adrenaline. Goal is to maintain MAP > 65mm Hg. Consider dobutamine in shock with evidence of cardiac dysfunction associated with persistent tissue hypoperfusion. Surviving Sepsis Campaign guidelines(48) doesn`t recommend dopamine in COVID-19 with shock possibly due to an increase risk of arrhythmias and lack of evidence of mortality benefit. These vasopressors should be titrated strictly to targeted blood pressure to maintain tissue perfusion and given preferably through a central venous catheter. When peripheral lines are used for infusion, watch for necrosis of skin or extravasation of vasopressors.
(6) Prone ventilation- If lung protective ventilation fails to maintain adequate oxygenation (PaO2/FiO2 < 150mm Hg despite PEEP >5 and FiO2 > 0.6), then prone ventilation should be considered. Guérin et al PROSEVA trial(53) reports promising results in patients with severe ARDS. It is a well-known fact that prone ventilation along with early NMB agents has improved survivability in ARDS(23). Prone ventilation also enhances oxygenation and decreases V/Q mismatch in ARDS patients. In COVID-19 patients' good response to prone positioning may be due to their well-preserved lung compliance compared with patients who develop ARDS from other causes. Therefore, patients are ventilated in prone position for at least 16 hours per day if patient fail to maintain oxygenation in supine position. However, utmost due care should be taken to avoid ventilator disconnections during position change, minimum staff should be kept for turning the patient to prone. Contraindications to prone ventilation (cervical spine injury, open chest, unstable airway, raised ICP, raised intraabdominal pressure) should be addressed prior to proning. It is imperative to mention that these patients should be well sedated to tolerate the tube and boluses of neuromuscular agents should be considered to avoid unnecessary coughing while turning to prone position. The optimal time and criteria to discontinue prone ventilation when PaO2/FiO2 >150mm Hg with FiO2 < 0.6 and PEEP < 10 cm H2O for at least 4 hours in supine position after a trial of prone position(54).
(7) Role of pulmonary vasodilators- The two most commonly used vasodilators in mechanically ventilated patients are inhaled nitric oxide gas (iNO) and epoprostenol. They are administered by continuous inhalation. Rescue therapy with them are considered to improve oxygenation when PaO2/FiO2 <100mm Hg despite prone ventilation or if it is associated with acute pulmonary arterial hypertension(48). If there is no improvement in oxygenation after instituting inhaled pulmonary vasodilators, then it should be tapered off without undue delay to avoid rebound pulmonary vasoconstriction. Epoprostenol has mild antiplatelet action, so it should be avoided in alveolar haemorrhage. The risk of aerosolization and clogging of HME filters is particularly more with Epoprostenol and it remains a concern in COVID-19 patients. That is why iNO is more preferred due to less frequent chance of filters and less risk of acquired infection in the HCWs. Routine use of inhaled nitric oxide in CARDS patients is not recommended as there is no evidence of survival benefit(48).
(8) Role of ECMO- If oxygenation doesn`t improve and hypoxia still persists then VV-ECMO (veno-venous extracor-poreal membrane oxygenation) can be considered subject to availability.
Indications of ECMO in COVID-19(55)- (a) PaO2/FiO2 >150 but pH <7.25 with PaCO2 >60 for more than 6 hours. (b) PaO2/FiO2 <80 mm Hg for 6 hours, PaO2/FiO2 <50 mm Hg for 3 hrs, and other adjunctive measures fail (prone position, NMB, recruitment manoeuvres, inhaled pulmonary vasodilators).
ECMO is expensive and extremely resource-limited treatment requiring trained personnel. Therefore, its use as rescue therapy should be considered only in refractory hypoxic respiratory failure(56). So far, no RCTs or meta-analyses have been conducted on ECMO in CARDS. Few reports from China mention ECMO instituted for CARDS, but their course of hospital stay, clinical course, and outcome were not discussed(57).
(9) Ventilator Weaning and extubation of CARDS patients- Special attention to avoid viral transmission to the health care providers during extubation in mandatory. Extubation is an aerosol generating procedure, so a high threshold for extubation should be kept for these patients to avoid unnecessary reintubation. Some physicians use cuff leak test criteria along with spontaneous breathing trials (SBT) to assess the readiness for weaning from mechanical ventilation on the assumption that these patients could have developed airway oedema due to prolonged ventilation. Since the risk of aerosol generation in cuff leak test is similar to extubation, it is advised to perform SAT (Spontaneous awakening trial) and SBT without T-piece at lower pressure support (0-3cm H2O) along with use steroids prior to extubation. The following weaning criteria is recommended prior to extubation(58)-
1. Patient should be conscious, comfortable, and oriented. 2. PaO2/FiO2 > 300 mm Hg with PEEP < 5 cm H2O. 3. Hemodynamically stable and maintaining SPO2 with FiO2 < 0.4. 4. RSBI (Rapid shallow breathing index) < 105 – calculated by respiratory rate/tidal volume in litres when the intubated patient is breathing spontaneously. 5. No signs of increase work of breathing or respiratory distress like use of accessory muscle, paradoxical or asynchronous respiration, nasal flaring, profuse diaphoresis, agitation, tachy-pnoea, tachycardia or cyanosis. 6. Good cough reflex with absence of expecto-ration/secretion.
Appendix 1 provides an algorithm for management of a patient with CARDS.
(10) Prevention of complications- Complications or adverse/side effects of mecha-nical ventilation should be prevented in all cases of CARDS, as with any other case of ARDS. Few of the interventions are enumerated below:
(a) Prevention of Ventilator Associated Pneumonia (VAP) (59) – VAP can be prevented by following: 1. Spontaneous awakening and spontaneous breathing trails. 2. Head of bed elevation. 3. Selective digestive decontamination. 4. Thromboprophylaxis. 5. Oral care without chlorhexidine as some patients develops ARDS due to aspiration of chlorhexidine. 6. Use a new ventilator circuit for each patient. 7. Change HMEs filter when soiled. 8. Oral intubation preferred compare to nasal intubation. (b) Reduce pressure sores and ulcers by frequent change of position every 2 hourly. (c) Reduce stress ulcer, gastric bleeding by early enteral feeding within 24-48 hrs of ICU admission and consider PPI or H2 blocker. (d) Reduce ICU related weakness by early mobilisation. (e) Reduce catheter related infection by using sterile aseptic technique while insertion and consider removal when not needed. (f) Reduce the number of days on mechanical ventilation by daily assessment for readiness of extubation through spontaneous breathing trials. (g) Reduce the incidence of venous thromboem-bolism by use of pharmacological agents or mechanical compression devices. (h) Suctioning of mechanically ventilated patients should be done with closed inline suction catheters to prevent aerosol spread and unnecessary ventilator disconnection should be avoided to prevent alveolar recruitment (32).
(11) Understanding recent advances in ARDS treatment- Salient features from various RCTs and clinical trials, that reflect recent advances and consensus in the understanding and management of ARDS-
(a) Multiple trials(60)(61) have failed to confirm the benefit of using recruitment manoeuvres in ARDS patients. (b) The LUNG-SAFE study(23)(62) - Shown increased mortality with noninvasive ventilation in severe ARDS patients. (c) Liberal oxygen or conservative oxygen (LOCO2) trial(63)- Conservative oxygenation strategy did not reveal increased survival benefits. So, hyperoxia (SpO2 >97%) and hypoxemia (SpO2 <90%) should be avoided. (d) SUPERNOVA study(64)- Use of extracorporeal carbon dioxide removal can be utilized to enable ultra-protective ventilation (Tidal volume= 4 mL/kg and PPLAT ≤ 25 cmH2O) in ARDS. (e) EOLIA trial(65)- Fails to approve the superiority of routine use of ECMO therapy in severe ARDS over rescue ECMO therapy.
For the transport of intubated patients, the use of evacuation pods have also been described for a medical evacuation (66).
Neuropsychiatric symptoms in cards Long-term outcomes of patients with ARDS are being increasingly recognized as important research targets, as many patients survive ARDS only to have ongoing functional and/or psychological sequelae.
The etiopathogenesis of neuropsychiatric manifestations could be either due to primary neuroinvasion by the coronavirus 2 (SARS-CoV-2) or a secondary attack of inflammation by activated immune and inflammatory mediators. The most common psychiatric presentation in ICU is of Delirium but other neurological symptoms such as rigidity, myoclonus, catatonia can also be encoun-tered.
Delirium- The prevalence of delirium in intubated patients is up to 80%(67) which is further exacerbated in CARDS patient. The risk factors include old age (>65yrs), medical co-morbidity, drugs (propofol, opiods, and high-dose benzo-diazepines, which are routinely used during mechanical ventilation), hydroxychloroquine (67,68).
Delirium can be objectively assessed and monitored with 'Confusion Assessment Method for the ICU' scale(69).
The management comprises of: 1. Regularizing the sleep cycle Melatonin should be used for regularizing sleep-wake cycle in delirium owing to its short half-life, additional mild anti-inflammatory properties and no respiratory depression (69). Benzodiazepines should be avoided (except in cases of delirium tremens), as cumulative doses run the risk of respiratory depression and may cause paradoxical disinhibition. Zolpidem (2.5-5mg) is relatively safer in terms of respiratory functioning, but levels are increased in patients taking ritonavir. 2. Acute agitation/Disruptive behaviour(70) Acutely disturbed behaviour can be managed with low dose antipsychotic drugs, however, monitoring of QTc interval, neurologic side effects (EPS), and sedation becomes essential. The risk of QTc prolongation gets further amplified, given the potential use of COVID-19–specific medica-tions that themselves prolong QTc (hydroxy-chloroquine, azithromycin), leading to a poten-tially increased risk of torsades de pointes(71). a) Haloperidol (2.5- 5mg) can be used orally or intramuscularly. Intravenous administration should be accompanied by ECG monitoring (70). b) Olanzapine 5-10 mg can also be considered either orally or parenterally. In an acutely disturbed patients, intramuscular (IM) is the preferred route of administration compared to intravenous (IV) route as it has minimal effect on QTc interval and lesser risk for EPS compared to haloperidol. c) Dexmedetomidine is alpha-2 agonist and reduces the release of noradrenaline and helps curtailing restlessness. Clonidine can also be used for the same reason and is more convenient as it's available in skin patches form. d) Valproic acid is known for its neuroprotective potential and can be used to control extreme emotional fluctuations. It also provides pro-phylaxis against the potentially epileptogenic state by increasing the seizure threshold. However, liver function tests and platelets need to be constantly monitored (58). e) In extreme cases not responding to the above measures, only short acting low dose oral benzodiazepines (e.g., lorazepam 1- 2 mg) may be considered with close monitoring for respiratory distress and respiratory failure.
Future Research CARDS unfortunately is still on the rise and our understanding on the progression and behaviour of the disease with respect to interventions is only becoming clearer day by day. Our meta-analysis suggests the recommendations that has been mentioned in the paragraphs above can be used a guide to curate management protocols by treating physicians. For each recommendation mentioned, it is important to consider the quality of the evidence reviews thoroughly before applying these recom-mendations to specific clinical situations or policy decisions. No guideline or recommendations can consider all the compelling clinical features of individual patients, as they are unique. However, it is also unknown whether similar results can be found in the unselected and broad population with critical illness. There is, thus, a great need for well designed, high-quality, large, randomized trials to confirm the effect of COVID-19 in critically ill patients with CARDS.
Conclusion
CARDS is an anticipated severe complication of COVID-19 that requires prompt recognition and comprehensive multi-speciality management. Extensive research and studies are required to address the vital unanswered queries about treatment of mechanically ventilated patients of CARDS. Because of the high mortality in mechanically ventilated patients, the above recommendations and findings direct the potential for improvement in the management of patients with CARDS.
Declarations: Ethics approval: Not applicable
Consent for publication The authors certify that they have obtained all appropriate patient consent forms in the written format, which can be made available to the journal. Availability of data and materials: Can be requested from the author SS: shibusasi@gmail.com
Competing interests None
Funding None
Authors' contributions Study conception and design: SS, VS, GKD Acquisition of data: VS, SS Analysis and interpretation of data: SS, VS, HSD, BM, GKD Drafting of manuscript: SS, AN Critical revision: SS, HSD, BM
Reference
1. Ferguson ND, Fan E, Camporota L, Antonelli M, Anzueto A, Beale R, et al. The Berlin definition of ARDS: An expanded rationale, justification, and supplementary material. Intensive Care Med [Internet]. 2012 [cited 2021 Mar 10]; 38(10): 1573–82. Available from: https://pubmed.ncbi.nlm.nih.gov/22926653/
2. GRADE approach | Cochrane Training [Internet]. [cited 2021 Mar 10]. Available from: https://training.cochrane.org/grade-approach
3. Li J, Fink JB, Ehrmann S. High-flow nasal cannula for COVID-19 patients: low risk of bio-aerosol dispersion [Internet]. Vol. 55, The European respiratory journal. NLM (Medline); 2020 [cited 2020 Jul 20]. Available from: https://doi.org/10.1183/13993003.00892-2020
4. Peng F, Tu L, Yang Y, Hu P, Wang R, Hu Q, et al. Management and Treatment of COVID-19: The Chinese Experience [Internet]. Vol. 36, Canadian Journal of Cardiology. Elsevier Inc.; 2020 [cited 2021 Mar 10]. p. 915–30. Available from: /pmc/articles/PMC7162773/
5. Ottestad W, Anaesthesia SS-BJ of, 2020 undefined. COVID-19 patients with respiratory failure: what can we learn from aviation medicine? bjanaesthesia.org [Internet]. [cited 2020 Jul 20]; Available from: https://bjanaesthesia.org/article/S0007-0912(20)30226-9/abstract
6. Bauer PR, Gajic O, Nanchal R, Kashyap R, Martin-Loeches I, Sakr Y, et al. Association between timing of intubation and outcome in critically ill patients: A secondary analysis of the ICON audit. J Crit Care. 2017 Dec 1;42:1–5.
7. Whittle JS, Pavlov I, Sacchetti AD, Atwood C, Rosenberg MS. Respiratory support for adult patients with COVID‐19. J Am Coll Emerg Physicians Open [Internet]. 2020 Apr 13 [cited 2021 Mar 10];1(2):95–101. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/emp2.12071
8. Nichani R, McGrath B, Nichani R, McGrath B. High-flow nasal cannula. In: OSCEs for the Final FFICM [Internet]. Cambridge University Press; 2016 [cited 2021 Mar 10]. p. 194–5. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526071/
9. Guérin C, Reignier J, Richard J-C, Beuret P, Gacouin A, Boulain T, et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N Engl J Med [Internet]. 2013 Jun 6 [cited 2021 Mar 10];368(23):2159–68. Available from: https://pubmed.ncbi.nlm.nih.gov/23688302/
10. Luo M, Cao S, Wei L, … RT-… : TJ of, 2020 undefined. Precautions for intubating patients with COVID-19. anesthesiology.pubs.asahq.org [Internet]. [cited 2020 Jul 20]; Available from: https://anesthesiology.pubs.asahq.org/article.aspx?articleid=2763451&_ga=2.110372871.388575457.1585001326-1917929588.1585001326
11. PPE-Info - Standard Details [Internet]. [cited 2021 Mar 10]. Available from: https://wwwn.cdc.gov/PPEInfo/Standards/Info/ANSI/AAMIPB70Class3
12. Meng L, Qiu H, Wan L, … YA-A, 2020 undefined. Intubation and Ventilation amid the COVID-19 OutbreakWuhan's Experience. anesthesiology. pubs. asahq.org [Internet]. [cited 2020 Jul 20]; Available from: https://anesthesiology.pubs.asahq.org/article.aspx?articleid=2763453
13. Preoxygenation - Anesthesia General [Internet]. [cited 2021 Mar 10]. Available from: https://anesthesiageneral.com/preoxygenation/
14. Sasidharan S, Goyal R, Babitha M, Singh S, Dhillon H. COVID aerosol barrier intubation box – Boon or bane? J Anaesthesiol Clin Pharmacol [Internet]. 2020 Aug 1 [cited 2021 Mar 10]; 36(5): 150. Available from: http://www.joacp.org/text.asp?2020/36/5/150/291182
15. Sasidharan S, Singh V, Dhillon H, Babitha M. Patient isolation pods for the evacuation of COVID-19 infected patients – Is this the answer? J Anaesthesiol Clin Pharmacol [Internet]. 2020 Aug 1 [cited 2021 Apr 7];36(5):152. Available from: http://www.joacp.org/text.asp?2020/36/5/152/291187
16. Oxygenation and Ventilation | COVID-19 Treatment Guidelines [Internet]. [cited 2021 Mar 10]. Available from: https://www.covid19treatmentguidelines.nih.gov/critical-care/oxygenation-and-ventilation/
17. Möhlenkamp S, Thiele H. Ventilation of COVID-19 patients in intensive care units [Internet]. Vol. 45, Herz. Springer Medizin; 2020 [cited 2021 Mar 10]. p. 329–31. Available from: https://doi.org/10.1007/s00059-020-04923-1
18. Roca O, Caralt B, Messika J, Samper M, Sztrymf B, Hernández G, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am J Respir Crit Care Med [Internet]. 2019 Jun [cited 2021 Mar 10];199(11):1368–76. Available from: https://www.atsjournals.org/doi/10.1164/rccm.201803-0589OC
19. Alhazzani W, Al-Suwaidan F, … ZAA-SCC, 2020 undefined. The saudi critical care society clinical practice guidelines on the management of COVID-19 patients in the intensive care unit. sccj-sa.org [Internet]. [cited 2020 Jul 20]; Available from: http://www.sccj-sa.org/article.asp?issn=2543-1854;year=2020;volume=4;issue=2;spage=27;epage=44;aulast=Alhazzani
20. Gattinoni L, Giosa L, Bonifazi M, Pasticci I, Busana M, Macri M, et al. Targeting transpulmonary pressure to prevent ventilator-induced lung injury [Internet]. Vol. 13, Expert Review of Respiratory Medicine. Taylor and Francis Ltd; 2019 [cited 2021 Mar 10]. p. 737–46. Available from: https://www.tandfonline.com/doi/abs/10.1080/17476348.2019.1638767
21. Walling P, Anaesthesia TS-BJ of, 1976 undefined. A comparison of oesophageal and central venous pressures in the measurement of transpulmonary pressure change. Elsevier [Internet]. [cited 2020 Jul 20]; Available from: https://www.sciencedirect.com/science/article/pii/S0007091217486958
22. Arentz M, Yim E, Klaff L, Lokhandwala S, Jama FR-, 2020 undefined. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State. jamanetwork.com [Internet]. [cited 2020 Jul 20]; Available from: https://jamanetwork.com/journals/jama/article-abstract/2763485
23. Nanchal R, F1000Research JT-, 2018 undefined. Recent advances in understanding and treating acute respiratory distress syndrome. ncbi.nlm.nih.gov [Internet]. [cited 2020 Jul 20]; Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6107983/
24. Meade MO, Cook DJ, Guyatt GH, Slutsky AS, Arabi YM, Cooper DJ, et al. Ventilation Strategy Using Low Tidal Volumes, Recruitment Maneuvers, and High Positive End-Expiratory Pressure for Acute Lung Injury and Acute Respiratory Distress Syndrome A Randomized Controlled Trial [Internet]. jamanetwork.com. [cited 2020 Jul 20]. Available from: https://jamanetwork.com/
25. Fan E, Beitler JR, Brochard L, Calfee CS, Ferguson ND, Slutsky AS, et al. COVID-19-associated acute respiratory distress syndrome: is a different approach to management warranted? Vol. 8, The Lancet Respiratory Medicine. Lancet Publishing Group; 2020. p. 816–21.
26. Gattinoni L, Chiumello D, Caironi P, Busana M, Romitti F, Brazzi L, et al. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Vol. 46, Intensive Care Medicine. Springer; 2020. p. 1099–102.
27. Gattinoni L, Quintel M, Marini JJ. LESS IS MORE IN INTENSIVE CARE “Less is More” in mechanical ventilation. Intensive Care Med [Internet]. 2020 [cited 2020 Jul 20];46:780–2. Available from: https://doi.org/10.1007/s00134-020-05981-z
28. Gattinoni L, Coppola S, … MC-A journal of, 2020 undefined. Covid-19 does not lead to a “typical” acute respiratory distress syndrome. atsjournals.org [Internet]. 2020 May 15 [cited 2020 Jul 20];201(10):1299–300. Available from: www.atsjournals.org.
29. Organization WH. Clinical management of severe acute respiratory infection when novel coronavirus ( nCoV) infection is suspected: interim guidance, 25 January 2020 [Internet]. 2020 [cited 2020 Jul 20]. Available from: https://www.who.int/health-topics/coronavirus
30. Robertson TE, Mann HJ, Hyzy R, Rogers A, Douglas I, Waxman AB, et al. Multicenter implementation of a consensus-developed, evidence-based, spontaneous breathing trial protocol*. Crit Care Med [Internet]. 2008 Oct [cited 2020 Jul 20];36(10):2753–62. Available from: http://journals.lww.com/00003246-200810000-00007
31. Chacko B, Peter J V., Tharyan P, John G, Jeyaseelan L. Pressure-controlled versus volume-controlled ventilation for acute respiratory failure due to acute lung injury (ALI) or acute respiratory distress syndrome (ARDS). Vol. 2017, Cochrane Database of Systematic Reviews. John Wiley and Sons Ltd; 2015.
32. AC-19 WG-: A and NZIC, 2020 undefined. The Australian and New Zealand Intensive Care Society (ANZICS)-COVID-19 Guidelines (Version 1).
33. Slutsky AS, Ranieri VM. Mechanical ventilation: Lessons from the ARDSNet trial. Vol. 1, Respiratory Research. 2000. p. 73–7.
34. Trasy D, Nemeth M, Kiss K, Till Z, Molnar Z. FiO2/PEEP index: a simple tool for opitimizing ventilator settings. Crit Care [Internet]. 2013 Apr 19 [cited 2020 Jul 20];17(S2):1–200. Available from: https://link.springer.com/articles/10.1186/cc12028
35. Möhlenkamp S, Thiele H. Ventilation of COVID-19 patients in intensive care units [Internet]. Vol. 45, Herz. Springer Medizin; 2020 [cited 2021 Mar 10]. p. 329–31. Available from: /pmc/articles/PMC7169372/
36. Zhang R, Wang X, Ni L, Di X, Ma B, Niu S, et al. COVID-19: Melatonin as a potential adjuvant treatment. Elsevier [Internet]. [cited 2020 Jul 20]; Available from: https://www.sciencedirect.com/science/article/pii/S0024320520303313
37. Jerath A, Ferguson ND, Cuthbertson B. Inhalational volatile-based sedation for COVID-19 pneumonia and ARDS. Intensive Care Medicine. Springer; 2020.
38. Jabaudon M, Boucher P, Imhoff E, Chabanne R, Faure J-S´ E, Roszyk L, et al. Sevoflurane for Sedation in Acute Respiratory Distress Syndrome A Randomized Controlled Pilot Study. Am J Respir Crit Care Med [Internet]. 2017 Mar 15 [cited 2020 Jul 20];195(6):792–800. Available from: www.clinicaltrials.gov
39. Shang Y, Pan C, Yang X, Zhong M, Shang X, Wu Z, et al. Management of critically ill patients with COVID-19 in ICU: statement from front-line intensive care experts in Wuhan, China. Vol. 10, Annals of Intensive Care. Springer; 2020.
40. Barr J, Gilles ;, Fraser L, Puntillo K, Wesley Ely ; E, Gélinas C, et al. Critical Care Medicine Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit. journals.lww.com [Internet]. 2013 [cited 2020 Jul 20]; Available from: www.ccmjournal.org
41. Rubulotta F, … HS-A-A and, 2020 undefined. Technologies to Optimize the Care of Severe Coronavirus Disease 2019 Patients for Health Care Providers Challenged by Limited Resources. ncbi.nlm.nih.gov [Internet]. [cited 2020 Jul 20]; Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7258840/
42. Kaplan L, Bailey H. Bispectral index (BIS) monitoring of ICU patients on continuous infusion of sedatives and paralytics reduces sedative drug utilization and cost. Crit Care. 2000;4(Suppl 1):P190.
43. Balas M, Weinhouse G, … LD-ROC, 2018 undefined. Interpreting and implementing the 2018 pain, agitation/sedation, delirium, immobility, and sleep disruption clinical practice guideline. journals.lww.com [Internet]. [cited 2020 Jul 20]; Available from: https://journals.lww.com/ccmjournal/FullText/2018/09000/Interpreting_and_Implementing_the_2018_Pain,.11.aspx
44. Papazian L, Aubron C, Brochard L, Chiche JD, Combes A, Dreyfuss D, et al. Formal guidelines: management of acute respiratory distress syndrome. Vol. 9, Annals of Intensive Care. Springer Verlag; 2019.
45. Mehta S, Burns KEA, Machado FR, Fox-Robichaud AE, Cook DJ, Calfee CS, et al. CRITICAL CARE PERSPECTIVE Gender Parity in Critical Care Medicine. Am J Respir Crit Care Med [Internet]. 2017 Aug 15 [cited 2020 Jul 20]; 17(4): 425–9. Available from: www.aamc.org/members/leadership/
46. Ho ATN, Patolia S, Guervilly C. Neuromuscular blockade in acute respiratory distress syndrome: A systematic review and meta-analysis of randomized controlled trials. J Intensive Care. 2020 Jan 28;8(1).
47. Yu IT, Hong Xie Z, Tsoi KK, Lan Chiu Y, Wai Lok S, Ping Tang X, et al. Why Did Outbreaks of Severe Acute Respiratory Syndrome Occur in Some Hospital Wards but Not in Others? Why SARS Outbreaks Occur Wards CID [Internet]. 2007 [cited 2020 Jul 20];1017. Available from: https://academic.oup.com/cid/article-abstract/44/8/1017/296620
48. Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving Sepsis Campaign: guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med [Internet]. 2020 [cited 2020 Jul 20];46:854–87. Available from: https://doi.org/10.1007/s00134-020-06022-5
49. Singh V, Sasidharan S, Nasser A, Dhillon H. Intubation and invasive Mechanical ventilation of COVID-19 Acute Respiratory Distress Syndrome patients. MRIMS J Heal Sci [Internet]. 2021 [cited 2021 Apr 7];9(1):21. Available from: http://www.mrimsjournal.com/text.asp?2021/9/1/21/312606
50. Barazzoni R, Bischoff S, Krznaric Z, Pirlich M. ESPEN expert statements and practical guidance for nutritional management of individuals with SARS-CoV-2 infection. 2020 [cited 2020 Jul 20]; Available from: https://www.sciencedirect.com/science/article/pii/S0261561420301400
51. Singer P, Blaser A, Berger M, nutrition WA-C, 2019 undefined. ESPEN guideline on clinical nutrition in the intensive care unit. Elsevier [Internet]. [cited 2020 Jul 20]; Available from: https://www.sciencedirect.com/science/article/pii/S0261561418324324
52. Ye XJ, Ji Y Bin, Ma BW, Huang DD, Chen WZ, Pan ZY, et al. Comparison of three common nutritional screening tools with the new European Society for Clinical Nutrition and Metabolism (ESPEN) criteria for malnutrition among patients with geriatric gastrointestinal cancer: A prospective study in China. BMJ Open [Internet]. 2018 Apr 1 [cited 2021 Mar 10];8(4):19750. Available from: http://bmjopen.bmj.com/
53. Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159–68.
54. Guérin C, Reignier J, … JR-… EJ of, 2013 undefined. Prone positioning in severe acute respiratory distress syndrome. Mass Med Soc [Internet]. [cited 2020 Jul 20]; Available from: https://www.nejm.org/doi/full/10.1056/nejmoa1214103
55. Fredericks AS, Bunker MP, Gliga LA, Ebeling CG, Ringqvist JRB, Heravi H, et al. Airway Pressure Release Ventilation: A Review of the Evidence, Theoretical Benefits, and Alternative Titration Strategies. Vol. 14, Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary Medicine. SAGE Publications Ltd; 2020.
56. MacLaren G, Fisher D, Jama DB-, 2020 undefined. Preparing for the most critically ill patients with COVID-19: the potential role of extracorporeal membrane oxygenation. jamanetwork.com [Internet]. [cited 2020 Jul 20]; Available from: https://jamanetwork.com/journals/jama/article-abstract/2761778
57. Yang X, Yu Y, Xu J, Shu H, Liu H, Wu Y, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Elsevier [Internet]. [cited 2020 Jul 20]; Available from: https://www.sciencedirect.com/science/article/pii/S2213260020300795
58. Subirà C, Hernández G, Vázquez A, Rodríguez-Garciá R, González-Castro A, Garciá C, et al. Effect of pressure support vs T-piece ventilation strategies during spontaneous breathing trials on successful extubation among patients receiving mechanical ventilation: A randomized clinical trial. JAMA - J Am Med Assoc [Internet]. 2019 Jun 11 [cited 2021 Apr 7]; 321(22): 2175–82. Available from: /pmc/articles/PMC6563557/
59. care MK-C opinion in critical, 2017 undefined. What is new in the prevention of nosocomial pneumonia in the ICU? journals.lww.com [Internet]. [cited 2020 Jul 20]; Available from: https://journals.lww.com/co-criticalcare/fulltext/2017/10000/what_is_new_in_the_prevention_of_nosocomial.5.aspx
60. Ferrando C, Blanco J. Open Lung Approach for the Acute Respiratory Distress Syndrome. ingentaconnect.com [Internet]. 2017 [cited 2020 Jul 20]; Available from: https://www.researchgate.net/publication/283748635
61. Walkey AJ, Sorbo L Del, Hodgson CL, Adhikari NKJ, Wunsch H, Meade MO, et al. SYSTEMATIC REVIEW Higher PEEP versus Lower PEEP Strategies for Patients with Acute Respiratory Distress Syndrome A Systematic Review and Meta-Analysis. Ann Am Thorac Soc [Internet]. 2017 Oct 1 [cited 2020 Jul 20];14:297–303. Available from: www.atsjournals.org
62. Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA [Internet]. 2016 [cited 2020 Jul 20];315(8):788–800. Available from: https://jamanetwork.com/
63. Barrot L, Asfar P, Mauny F, Winiszewski H, Montini F, Badie J, et al. Liberal or conservative oxygen therapy for acute respiratory distress syndrome. N Engl J Med. 2020 Mar 12;382(11):999–1008.
64. Combes A, Fanelli V, Pham T, Ranieri VM, Goligher EC, Brodie D, et al. Feasibility and safety of extracorporeal CO 2 removal to enhance protective ventilation in acute respiratory distress syndrome: the SUPERNOVA study. Intensive Care Med. 2019 May 1;45(5):592–600.
65. Combes A, Hajage D, Capellier G, Demoule A, Lavoué S, Guervilly C, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018 May 24;378(21):1965–75.
66. Sasidharan S, Singh V, Dhillon H, Babitha M. Patient isolation pods for the evacuation of COVID-19 infected patients - Is this the answer? [Internet]. Vol. 36, Journal of Anaesthesiology Clinical Pharmacology. Wolters Kluwer Medknow Publications; 2020 [cited 2021 Mar 10]. p. S152–5. Available from: /pmc/articles/PMC7574020/
67. Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE, et al. Delirium as a Predictor of Mortality in Mechanically Ventilated Patients in the Intensive Care Unit. J Am Med Assoc [Internet]. 2004 Apr 14 [cited 2021 Mar 10];291(14):1753–62. Available from: https://jamanetwork.com/
68. Maldonado JR. Delirium pathophysiology: An updated hypothesis of the etiology of acute brain failure. In: International Journal of Geriatric Psychiatry. John Wiley and Sons Ltd; 2018. p. 1428–57.
69. Evaluation of delirium in critically ill patients: Validatio... : Critical Care Medicine [Internet]. [cited 2021 Mar 10]. Available from: https://journals.lww.com/ccmjournal/Abstract/2001/07000/Evaluation_of_delirium_in_critically_ill_patients_.12.aspx
70. Dhillon H, Sasidharan S, Dhillon G, Singh V, Babitha M. COVID-19: Neuropsychiatric manifestations and psychopharmacology. Ann Indian Psychiatry [Internet]. 2020 [cited 2021 Mar 10];4(2):226. Available from: http://www.anip.co.in/text.asp?2020/4/2/226/301441
71. Roden DM, Harrington RA, Poppas A, Russo AM, Russo AM. Considerations for drug interactions on QTc in exploratory COVID-19 treatment [Internet]. Vol. 141, Circulation. Lippincott Williams and Wilkins; 2020 [cited 2021 Mar 10]. p. E906–7. Available from: https://www.elsevier.com/__data/assets/pdf_file/0004/996745/MCP_Pos-
This work is under a Licencia Creative Commons