Revista Peruana de Investigación en Salud, ISSN: 2616 - 6097 https://doi.org/10.35839/repis.5.3.892
Appropriateness of colonoscopy indication according to EPAGE II criteria in a Uruguayan university hospital
Adecuación de la indicación de la colonoscopia según criterios de EPAGE II en un hospital universitario de Uruguay
Rodrigo Dorelo1,a, Soledad Francia1,b, Joaquín Berrueta1,c, Alicia Aleman2,d, Carolina Olano1,e
1Clínica de Gastroenterología “Prof. Dra. Carolina Olano”, Facultad de Medicina, Universidad de la República, Uruguay
2Departamento de Medicina Preventiva y Social, Universidad de la República, Montevideo, Uruguay
Correspondence: E-mail:digo.castaldelli@gmail.com
Orcid ID: ahttps://orcid.org/0000-0001-8516-3973, bhttps://orcid.org/0000-0001-9520-9824, chttps://orcid.org/0000-0002-1579-5032, dhttps://orcid.org/0000-0002-9247-1031, ehttps://orcid.org/0000-0002-4340-4051
Received December 23, 2020
Accepted for publication: May 24, 2021
Abstract
Background: Prioritization of criteria have been developed to reduce the increased demand. The European Society for Gastrointestinal Endoscopy developed an online program (EPAGE II). The aim of this study is to evaluate the appropriateness of the colonoscopy indication according to the EPAGE II criteria and correlate it with the endoscopic findings. Materials and Methods: Retrospective and analytical study that included all colonoscopies performed in the period March 2018 - March 2019. Colonoscopies with insufficient preparation and missing data, were excluded. They were categorized into having appropriate, inappropriate and uncertain indication, according to EPAGE II criteria. Sociodemographic data, indication, degree of preparation, and the presence of relevant findings were recorded. Results: 648 studies were included, 64.7% were women, and 51.8% were ordered by gastroenterologists. In 62% the preparation was adequate. In 171 (26.4%) the indication was CCR screening. In 525 (81%) the indication was appropriate, in 79 (12,2%) was not appropriate and in 44 (6,8%) was uncertain. An appropriate indication was significantly associated with age older than 50 years (p≤0.001). An endoscopic relevant diagnosis was observed in 55.2%. There was a significant association between appropriate indication and a relevant endoscopic diagnosis (p <0.01). The sensitivity, specificity, PPV and NPV of EPAGE II for an appropriate indication in relation to a relevant endoscopic finding were 84.92 %, 24.14%, 69.72% and 43.75% respectively. Conclusions: In this group of patients the EPAGE II showed high sensitivity and low specificity for the appropriateness of the indication in relation to the findings.
Keywords: appropriateness, colonoscopy, EPAGE II.
Resumen
Antecedentes: Criterios de priorización han sido desarrollados para disminuir el aumento de la demanda en las unidades de endoscopía. Se ha creado la guía europea sobre la idoneidad de la endoscopía gastrointestinal (EPAGE II). El objetivo de este estudio es evaluar la adecuación de la indicación de colonoscopia según los criterios de la EPAGE II y correlacionarla con los hallazgos endoscópicos. Materiales y Métodos: Estudio retrospectivo y analítico que incluyó todas las colonoscopias realizadas en el período marzo 2018 - marzo 2019. Se excluyeron las colonoscopias con preparación insuficiente y falta de datos. Se clasificaron en indicación apropiada, inapropiada e incierta, de acuerdo con los criterios de EPAGE II. Se registraron datos sociodemográficos, indicación, grado de preparación y presencia de hallazgos relevantes. Resultados: se incluyeron 648 estudios, 64,7% fueron mujeres y 51,8% fueron pedidos por gastroenterólogos. En 62% la preparación fue adecuada. En 171 (26,4%) la indicación fue cribado CCR. En 525 (81%) la indicación fue adecuada, en 79 (12,2%) no fue adecuada y en 44 (6,8%) fue incierta. Una indicación adecuada se asoció significativamente con la edad mayor de 50 años (p≤0,001). Se observó un diagnóstico endoscópico relevante en 55,2%. Hubo una asociación significativa entre la indicación apropiada y un diagnóstico endoscópico relevante (p <0.01). La sensibilidad, especificidad, VPP y VPN de EPAGE II para una indicación adecuada en relación con un hallazgo endoscópico relevante fueron 84,92%, 24,14%, 69,72% y 43,75% respectivamente. Conclusiones: En este grupo de pacientes EPAGE II mostró alta sensibilidad y baja especificidad para la correcta adecuación de la indicación para los hallazgos en VCC en general.
Keyword: adecuación, colonoscopia, EPAGE II.
Introduction
In the last few years, the demand of endoscopy procedures has increased, generating a significant increment in health costs and in waiting time (1).
Nowadays, colonoscopy represents the best technique available to provide screening and surveillance of colo-rectal cancer (CRC) and for the diagnosis and treatment of different colon diseases. Therefore, it has become a usual and massive procedure (2, 3).
It is the first line test for most patients with intestinal symptoms, iron deficiency anemia, radiological findings, positive fetal occult blood test (FOBT), surveillance post polypectomy or post CRC, evaluation of inflammatory bowel disease (IBD) patients, suspicion of abdominal masses, etc (1, 2, 4).
In Uruguay, such as in many other countries, endoscopy units perform open access endoscopy (OAE). OAE allows general practitioner to refer patients to endoscopy without prior consultation of Gastroenterologist.
Many scientific societies guidelines have established criteria to evaluate the appropriateness of the endoscopy indication. These criteria would help the practitioners in making proper decisions, increasing the quality of their practices and the adequate usage of medical resources. A group of experts elaborated the “European Panel on the Appropriateness of Gastrointestinal Endoscopy” (EPAGE) (5), a guideline that establishes the appropriateness of the indication based on some parameters (age, alarm symptoms, previous colonoscopies, previous treatments, etc). The guideline was subsequently updated to the current version, is the EPAGE II.
EPAGE II was validated by many studies from different countries in order to decrease the inappropriate indication in colonoscopy (6, 7, 8).
The main aim of this study was to evaluate the appropriateness of the indication in colonoscopy in a university endoscopy unit in Uruguay.
The secondary aim was to correlate the appropriateness of the indication to the relevant endoscopy findings.
Methods
A retrospective analytical study was performed. All colonoscopies performed in the period March 2018 - March 2019 in the Hospital de Clinicas “Manuel Quintela”, a university hospital from Montevideo, Uruguay, were included. Colonoscopies with insufficient preparation (by endoscopy report) or with missing data in selected variables, were excluded.
The following variables were considered: gender, age, referral physician or department (gastroenterologists, surgeons, medical practitioners, emergency), indication, colon preparation (according to the report) and colonoscopy findings. Colonoscopy findings were categorized into relevant findings (CRC, polyps, IBD, angiodysplasia and benign stenosis) and non-relevant findings (all others).
According to EPAGE II criteria, the indications were categorized into: appropriate (7-9 points), non-appropriate (1-3 points) and uncertain (4-6 points).
Statistical analysis Descriptive analysis was performed for sociodemographic, clinical and referral features. The appropriateness of the indication was related to the type of indication of the study, the demographic characteristics of the participants and the type of professional that indicated the study. The statistical association was evaluated with X2 tests for the qualitative variables (level of significance p ≤ 0.05). Sensitivity, specificity and positive and negative predictive value and 95% confidence intervals of an adequate indication for the diagnosis of pathologies in general and relevant pathologies were also analyzed. The statistical package SPSS (version 15.0) was used to make analysis.
Ethical disclosures Written informed consent was obtained from all patients prior to perform the colonoscopy.
Results
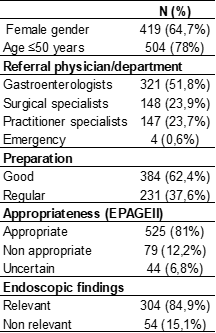
981 colonoscopy reports were revised, 648 fulfilled inclusion criteria. 64,7% were women, mean age 59 +/- 14 years. Socio demographic data, indications, preparation, referral physician/department, appropriateness of the indication (EPAGE II) and endoscopic findings are shown in Table 1.
Table 1 – Sociodemographic data, indications, preparation, referral physician/department, appropriateness of the indication (EPAGE II) and endoscopic findings
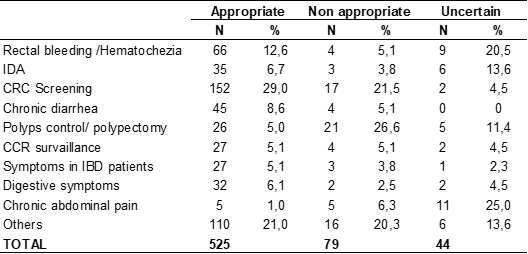
Table 2 shows the appropriateness of the indication according to the referral indication. 79 indications were non-appropriate, the most frequent were: post polypectomy surveillance (26,6%) and CRC screening (21,5%), when indicated in inadequate patients or incorrect time period.
Table 2. Appropriateness of the indication according to pretest pathology/symptoms
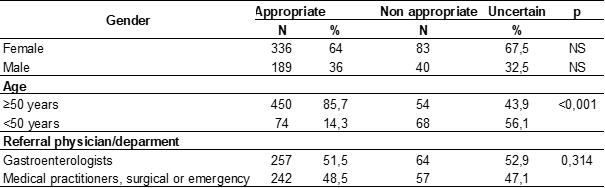
An association between the appropriate indication and age older than 50 years was observed (p≤0,001). No association between the appropriate indication and gender or the referral physician/ department was observed. See Table 3.
Table 3. Appropriateness of the indication vs age, gender, referral physician/department
Endoscopic findings were found in 435 (67,1%) colonoscopies, 358 (55,2%) of them were relevant. 304 (84,9%) of the relevant findings were conside-red appropriated. A significant association between the appropriateness of the indication and a relevant endoscopic finding was observed (p0,01)
Sensibility, specificity, PPV and NPV of EPAGE II for the appropriateness of the indications related to findings are shown in Table 4.
Table 4. Sensibility, specificity, PPV and NPV of EPAGE II for the appropriateness of the indications related to findings
Discussion
Endoscopy has an essential role in the diagnosis and treatment of patients with digestive diseases. The appropriateness of the indication is a key issue to reduce the waiting list, avoiding the delay for those with a potential malignant disease. Several guidelines have been developed to check the appropriateness of the referral based on a series of variables (age, gender, referral physician/department, indication, etc.)
In this study, according to the EPAGE II criteria, 12% of the indications were inappropriate, lower than the reported by Carrión et al (18%) (1). Other study, using EPAGE I showed that 23% of the colonoscopies had inappropriate indication (7).
In concordance with other international studies, in this group of patients, the most frequent inappropriate indications were the post polypectomy surveillance and CRC screening when indicated in inadequate patients or incorrect time (1, 7, 9). This can be explained to a lack of adhesion to the international screening and surveillance guidelines (10, 11).
The most frequent indication in our series, with 78% of patients with age older than 50 years, was CRC screening followed by rectal bleeding/hemato-quezia. The detection of pre-malignant lesions and CRC in early stages, using screening campaigns, is the most effective measure that significantly reduce the cancer incidence and mortality rates. Worldwide a noninvasive test for the average risk population screening is used. In Uruguay, the CRC is a leading cause of death and its screening is offered to all individuals with average risk factors over 50 years of age (10, 11). In our study, as in several others, CRC screening is the most frequent indications, whereas in a Spanish study of Fernández-Esparrach et al, the majority of colonoscopies were performed for diagnosis purposes, which was justified by the authors due to the high percentage of patients being referred by primary care physicians (1,8).
A significant association between appropriate indication and age older than 50 years was found. The CRC diagnosis in asymptomatic patients from 40 to 49 years of age using colonoscopy is unusual. The low diagnostic yield of the screening with colonoscopy on this group of age is consistent with current guidelines recommendations for the age of onset in average risk population (12).
In four patients with rectal bleeding, the indication was not adequate according to the EPAGE criteria given that the patients were under 50 years of age, had no risk factors for CRC, had a recent exploration with sigmoidoscopy for this bleeding episode and a colonoscopy within last 5 years assumed normal.
In our study, EPAGE II criteria showed high sensibility and low specify for the appropriateness of the indication in relation to relevant endoscopic findings.
Taking into account the low specificity of this criteria, exclusion of relevant lesions in patients with inappropriate indication cannot be guaranteed. Therefore, this should be considered a limitation of the program. In other study a high specificity and low sensibility was found but in a series with low number of patients (1).
From our results, we can affirm that EPAGE II is a practical and didactic tool that allows a fast decision making on what indication is adequate, in order to perform an efficient usage of colonoscopy. Even though we considered that some indications that we considered are adequate, are not included in this program, such as: symptomatic patients with HIV/Aids and the etiological search of a chronic diarrhea.
Some technical limitations were also found in the program. In the option with corresponding to the CRC surveillance in IBD patients the program does not allow to continue entering data and the option is blocked. In other options, the program allows the selection of only one option, avoiding the appropriateness evaluation.
As an interesting fact, in this study a considerable number of colonoscopies were performed with “presurgical evaluation of abdominal wall hernia” as an indication, that is not considered appropriate in most of the international guidelines. In a previous paper we have found a low CRC incidence in this population (13). These results were in accordance to other international studies and no evidence that colonoscopy is needed in the pre-surgery evaluation in these patients (14, 15, 16). This shows that even surgeons inappropriately indicates this procedures as well the rest of the physicians.
As a strength, this is the first national study on the usage of a tool that evaluates the appropriateness of the indication of colonoscopy and to our knowledge this is the study with the largest number of patients in the validation of EPAGE II. As a limitation, it is a retrospective study and the absence of a unique criteria for colonoscopy preparation, which led to the exclusion of 333 patients.
If the technical problems on the program are solved, it would be interesting to perform a new study to reevaluate its diagnostic accuracy (mainly its specificity) and, therefore promote its usage on the daily practice.
Conclution
In this group of patients, the EPAGE II showed high sensitivity and low specificity for the appropriateness of the indication in relation to the findings. This makes it a potentially useful tool to re-evaluate the correct indication, decreasing unnecessary colonoscopies and unsatisfied demand.
Conflict of interest
The authors declare that there is no conflict of interest.
Financial disclousure
No specific grants were received from public sector agencies, the business sector, or non-profit organizations in relation to this study.
Bibliographic references
1. Carrion S, Marin I, Lorenzo-Zuniga V, et al. [Appropriateness of colonoscopy indications according to the new EPAGE II criteria]. Gastroenterología y hepatología. 2010; 33(7): 484-489.
2. Vázquez-Iglesias JL, Alonso Aguirre PA, Duranas Vilas J. Endoscopia Digestiva Diagnóstica y Terapéutica. Colonoscopia. Madrid. Edit. Panamericana; 2009.p.115-147.
3. Blero D, Devière J. Endoscopic complications--avoidance and management. Nature reviews Gastroenterology & hepatology. 2012;9(3):162-172.
4. Fisher DA, Maple JT, Ben-Menachem T, et al. Complications of colonoscopy. Gastrointestinal endoscopy. 2011;74(4):745-752.
5. Vader JP, Froehlich F, Dubois RW, et al. European Panel on the Appropriateness of Gastrointestinal Endoscopy (EPAGE): conclu-sion and WWW site. Endoscopy. 1999: 31(8): 687-694.
6. Arditi C, Peytremann-Bridevaux I, Burnand B, et al. Appropriateness of colonoscopy in Europe (EPAGE II). Screening for colorectal cancer. Endoscopy. 2009;41(3):200-208.
7. Balaguer F, Llach J, Castells A, et al. The European panel on the appropriateness of gastrointestinal endoscopy guidelines colonoscopy in an open-access endoscopy unit: a prospective study. Alimentary pharmacology & therapeutics. 2005;21(5):609-613.
8. Fernández-Esparrach G, Gimeno-García AZ, Llach J, et al. Guidelines for the rational use of endoscopy to improve the detection of relevant lesions in an open-access endoscopy unit: a prospective study. Medicina clínica. 2007; 129(6): 205-208.
9. Gimeno-Garcia AZ, Quintero E. Colonoscopy appropriateness: Really needed or a waste of time? World journal of gastrointestinal endos-copy. 2015;7(2):94-101.
10. Guía de práctica clínica de tamizaje del cáncer colo-rectal. Ministerio de salud pública del Uruguay; 2018. https://www.gub.uy/ministerio-salud-publica/sites/ministerio-salud-publica/files/documentos/publicaciones/Gu%C3%ADa%20para%20el%20tamizaje%20del%20cáncer%20colo-rectal.pdf
11. Rex DK, Johnson DA, Anderson JC, et al. American College of Gastroenterology guidelines for colorectal cancer screening 2009 [corrected]. The American journal of gastroen-terology. 2009;104(3):739-750.
12. Imperiale TF, Wagner DR, Lin CY, et al. Results of screening colonoscopy among persons 40 to 49 years of age. The New England journal of medicine. 2002; 346(23):1781-1785.
13. Machado P, Berrueta J, Sangunetti A, et al Prevalencia de cáncer colorrectal en pacientes en valoración preoperatoria de hernia de pared abdominal. Rev Méd Urug 2015; 31(4):259-264.
14. Gerson LB, Triadafilopoulos G. Is colorectal cancer screening necessary in the preoperative assessment of inguinal herniorrhaphy? A case-control study. The American journal of gastroen-terology.2001; 96(6):1914-1917.
15. Avidan B, Sonnenberg A, Bhatia H, et al. Inguinal hernia is not a sign of colon cancer: results of a prospective screening trial. Alimen-tary pharmacology & therapeutics. 2002; 16(6):1197-201.
16. Samarakoon, Y., Gunawardena, N., Pathirana, A. et al. “Appropriateness of colonoscopy according to EPAGE II in a low resource setting: a cross sectional study from Sri Lanka”. BMC Gastroenterol. 2018; 18 (72).
This work is under a Licencia Creative Commons